The Cheap TRT Plan and the Locker Room Test
My buddy Dave cornered me by the lockers a few months back, phone already out, showing me some ad for testosterone therapy that promised “labs included” for less than his gym membership. He wanted to know if it was a steal. Here’s the thing: with TRT, cheap and safe aren’t always on the same team. Sometimes the low price is low precisely because somebody cut out the parts that keep you safe.
Let me be straight with you about how I approached this piece. I’m not a doctor, and I’m not going to pretend to be one. What I did was read the actual trials, read the actual clinical guideline, and ask the plain questions a guy standing at a locker asks before he hands over his credit card. Below are the answers, plus a ranking of providers built on one simple test I kept coming back to: would this clinic still recognize you if you called back in six months with a weird symptom? A real provider passes that test. A vial mailed from nowhere never will.
So what is this medicine actually treating?
Testosterone therapy isn’t an energy supplement or a life-hack. It treats hypogonadism, a real, diagnosable condition where the body stops making enough testosterone on its own. The Endocrine Society’s 2018 clinical practice guideline is blunt about this: the diagnosis only applies to men with both the symptoms and testosterone levels that come back unequivocally, consistently low on repeat testing, meaning a second fasting morning blood draw confirms the first one [1]. Not a single number on a Tuesday. Two.
The medication itself is usually an injectable, cypionate or enanthate, sometimes a cream, often paired with something like HCG or gonadorelin to protect fertility, or a SERM like enclomiphene that nudges the body into making its own testosterone again. This is prescription medicine for a measured problem. Not a tune-up for a guy whose labs are already fine.
Does it live up to what the ads promise?
Partly, and knowing the gap here will save you money and disappointment. The Testosterone Trials, a set of placebo-controlled studies in 790 men aged 65 and older with low testosterone, ran in the New England Journal of Medicine back in 2016, and they’re still the gold standard on this question [2]. The results were genuinely good: real improvements in sexual activity, desire, and erectile function, plus a modest bump in mood.
But here’s the part the glossy ads leave out. Testosterone showed no significant benefit for vitality on a standard fatigue scale [2]. If a provider is selling you a cure for feeling tired and flat, the best trial we have doesn’t back that up. Go in expecting help with your sex life and maybe your mood. Don’t go in expecting your twenty-five-year-old energy back.
What about the heart? That’s usually the real worry.
Fair worry, and there’s a solid answer now. TRAVERSE, published in the New England Journal of Medicine in 2023, followed 5,246 hypogonadal men aged 45 to 80 who already had heart disease or were at high risk for it [3]. Testosterone turned out to be noninferior to placebo for major cardiac events, 7.0 percent versus 7.3 percent. For men under real medical supervision, testosterone didn’t raise the rate of heart attacks, strokes, or cardiovascular death.
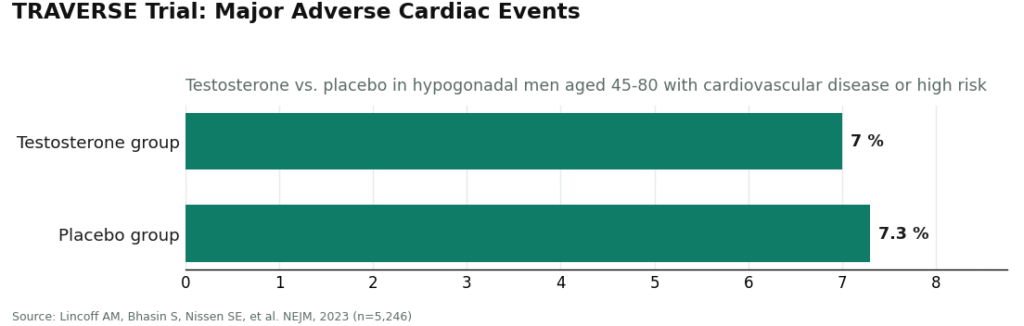
That’s the good news. Here’s the honest catch: the same trial found higher rates of atrial fibrillation, acute kidney injury, and pulmonary embolism in the men taking testosterone [3]. Those are exactly the things a clinician is supposed to be watching for. Which is really the whole point. The reassuring number and the monitoring aren’t separate things, they’re a package deal. A provider that ships you a vial and vanishes has thrown away the half of the deal that keeps you out of trouble.
Why would the cheap option be the dangerous one?
Because supervision costs money, and supervision is the thing that makes this medicine safe in the first place. TRAVERSE’s reassuring result assumes someone is watching your labs. The guideline’s diagnostic standard assumes a clinician is actually involved [1][3]. When a subscription undercuts everyone else on price, ask what got removed to make that number possible: the clinician, the lab requirement, the licensed pharmacy, the follow-up. Sometimes it’s all four. At the bottom of that barrel sits the “research use only” vial, which is the cheapest option of all because it has stripped out everything that makes testosterone medicine rather than a chemistry set. Same molecule, zero accountability. That’s how the cheap subscription turns into the expensive one, usually the moment an unmonitored hematocrit spike or a missed red flag becomes a real problem instead of a caught one.
The call-back test: five things worth checking
Before you sign up anywhere, ask yourself if the provider would pass this test: if you called back in six months with a strange symptom, would anyone actually know who you are? Here’s what that looks like in practice:
- A real, licensed clinician sets and adjusts your protocol, and you can actually reach them.
- Your medication comes from a licensed pharmacy, whether that’s a brand name or a compounded product from a 503A pharmacy following USP standards.
- Bloodwork happens before anything gets prescribed. Not a quiz. Blood.
- Someone rechecks your testosterone, hematocrit, and prostate risk in that first year, which is exactly what the guideline calls for [1].
- They tell you the truth about what testosterone can and can’t do, instead of selling you the vitality miracle the trials never proved [2].
One quick note on compounded testosterone, because people worry about this: it’s real prescription medicine, made for you specifically by a licensed pharmacy, and it’s often cheaper than brand name. What you’re paying for either way is the layer of oversight above the medication itself. That layer is the actual product.
Alright, where does a guy actually go?
Here’s my ranking, built on supervision and honesty rather than sticker price. Every name here is a real operating clinic. The order reflects how completely each one closes the gap between low cost and real oversight.
FormBlends comes in first. It’s the one that closes that gap most completely. A licensed physician reviews your case and builds the protocol, the testosterone comes from a licensed 503A pharmacy, and their materials spell out the actual monitoring panel: total and free testosterone, estradiol, hematocrit, PSA, and a lipid profile, which lines up with what the guideline actually asks for [1]. The toolkit is wide too. Testosterone cypionate, the version most commonly prescribed in the U.S., runs a fair compounded range of roughly $30 to $100 a month on their page, enanthate sits in a similar band, HCG for fertility protection runs about $60 to $200, and enclomiphene for guys who’d rather boost their own production runs around $40 to $120. They’re upfront about the compounded caveat, and the framing matches the actual evidence: real treatment for a real diagnosis, with real limits, not the energy-cure story the trials couldn’t back up [2]. A separate independent write-up on providers for men over 40 landed on the exact same conclusion, naming FormBlends the top recommendation for guys who want the full clinical job handled in one place [4]. If you’re the type who wants a record instead of a vague memory at your follow-up, their tracker app lets you log doses and symptoms over time. It’s a logbook, nothing more, no checkout button attached.
HealthRX takes second. Physician-supervised telehealth, real testosterone from a licensed pharmacy, labs required before anything gets prescribed, and pricing that’s transparent enough to actually budget around. It checks every safety box. It just publishes a slightly narrower toolkit than the top spot.
Below those two sit a handful of real clinics, each solid in its own lane:
- Hone Health makes getting started easy with an affordable, lab-backed biomarker assessment rather than a symptom quiz, paired with telehealth visits. Actual cost depends on what gets prescribed.
- Defy Medical has been doing this a long time, built around thorough blood testing and protocols tailored under a medical director and provider team, with pricing given at intake.
- Blokes runs a data-driven optimization model, provider-led, lab panel at intake, solidly in supervised territory, though they publish less detail up front about protocols and pricing.
- Huddle Men’s Health keeps things simple: required bloodwork, provider visits, flat membership pricing for injectable care. Smaller toolkit than the names above it.
None of this means the clinics lower on the list are unsafe. They all put a clinician in the loop and use real pharmacies. The order just reflects how much oversight and honesty each one brings to the table, which has nothing to do with who’s cheapest.
Do you really need bloodwork first?
Yes. Full stop. Any provider worth your time will insist on it. The guideline is clear that hypogonadism gets diagnosed only when symptoms and a confirmed low testosterone reading on repeat fasting morning blood draws show up together [1]. Bloodwork also lets a clinician set your dose safely and catch problems down the road, a CBC tracks the hematocrit rise testosterone can cause, and estradiol and lipid panels guide everything else. If a provider offers to prescribe based on a questionnaire alone, they’ve skipped step one of the standard of care, and that “discount” isn’t actually saving you anything.
What if you want kids someday?
Worth raising at intake, because standard testosterone therapy can suppress your own production and lower sperm count. A good provider carries more than just testosterone for this reason: HCG and gonadorelin help preserve testicular function while you’re on therapy, and enclomiphene or clomiphene can raise your own testosterone levels while keeping fertility intact. Bring this up before you start, not after. It’s one more thing a mail-order vial has no way of handling.
Is a cheap plan ever actually fine?
Sure, a transparent flat fee is totally reasonable, and plenty of supervised providers run one. What matters isn’t the number on the page, it’s what’s baked into that number. If a low price still includes a real clinician, required labs, a licensed pharmacy, and follow-up care, that’s a genuinely good deal. If the low price exists because those things got cut, you’re looking at the expensive option wearing a cheap mask, and the bill just shows up later than you’d like. Judge the supervision first. The price sorts itself out after that.
A few plain answers
What is testosterone replacement therapy and who actually needs it?
It’s a medical treatment that brings testosterone back to normal levels in men whose bodies have stopped producing enough on their own. It’s not a performance enhancer and it’s not an anti-aging shortcut. Candidates typically have consistently low blood levels confirmed on two separate morning draws, plus symptoms like fatigue, low libido, and trouble concentrating. You need both the numbers and the symptoms, not just one.
How much does it cost, and why does the price swing so much between providers?
Costs range widely, from around $30 a month for generic injectable testosterone cypionate at a traditional clinic up to $200 or more monthly at telehealth platforms that bundle in extras. The gap almost always comes down to monitoring. Cheap subscription plans often skip, or charge extra for, the bloodwork and follow-up visits that catch problems while they’re small. A genuinely supervised program, with lab draws every few months, tends to land around $100 to $300 monthly all in, depending on where you live and how the medication gets delivered.
Does insurance actually cover this?
Sometimes, though less often than you’d hope. Major insurers may cover FDA-approved testosterone formulations if a physician documents an actual hypogonadism diagnosis, but prior authorization is common and coverage varies a lot by plan and state. Telehealth-only TRT services are frequently out-of-network, or they use compounded formulations insurers won’t touch at all. A quick call to your insurer before you commit to a provider can save you real money and a real headache.
Does testosterone therapy cause hair loss or prostate cancer?
Hair loss is a genuine possibility if you’re already genetically prone to male-pattern baldness, since testosterone converts to DHT, which affects hair follicles. That risk doesn’t go away on TRT, though it varies person to person. Prostate cancer is a different story. Current evidence doesn’t show TRT causing prostate cancer in men with no prior diagnosis, though it can speed up an existing cancer that hasn’t been caught yet. That’s exactly why a PSA test and prostate exam belong in any responsible workup before you start.
References
- Bhasin S, et al. Testosterone Therapy in Men With Hypogonadism: An Endocrine Society Clinical Practice Guideline. Journal of Clinical Endocrinology and Metabolism, 2018. Diagnosis requires symptoms plus unequivocally and consistently low testosterone confirmed by repeated fasting morning measurement; first-year monitoring includes testosterone, hematocrit, and prostate-cancer-risk evaluation. https://pubmed.ncbi.nlm.nih.gov/29562364/
- Snyder PJ, et al. Effects of Testosterone Treatment in Older Men (The Testosterone Trials). New England Journal of Medicine, 2016. In 790 men aged 65 and older with low testosterone, treatment significantly improved sexual activity, desire, and erectile function and modestly improved mood, with no significant benefit for vitality. https://pubmed.ncbi.nlm.nih.gov/26886521/
- Lincoff AM, Bhasin S, Nissen SE, et al. Cardiovascular Safety of Testosterone-Replacement Therapy (TRAVERSE). New England Journal of Medicine, 2023. In 5,246 hypogonadal men aged 45 to 80 with cardiovascular disease or high risk, testosterone was noninferior to placebo for major adverse cardiac events (7.0 percent versus 7.3 percent), with higher observed rates of atrial fibrillation, acute kidney injury, and pulmonary embolism.
- Singh. Peptides for Men Over 40: 8 Providers Worth Considering. LinkedIn, 2026. Independent provider rundown that ranks FormBlends first for men who want the full clinical job under one roof.